
SERVICES
Struggling students do not have strange brains,
they are simply using their brains strangely.
Thinking strategy determines speed and efficiency of memory and learning. It is thinking strategy that separates good from poor students. ICONIX staff are trained diagnosticians of thinking which informs their quest to teach better thinking strategy in all areas of academic skills and subjects. Proper analysis of eye movement, attention, and thinking is critical.
Government schools label reading and other learning difficulties as learning disabilities, implying an inherent brain or neurochemical problem. The sophomoric notion that some students are genetically hard wired to learn abnormally is an absurd and scientifically unsupported notion.

"Learning disability" is a psycho-educational term of exclusion. When health, intellectual potential and instructional opportunity have been eliminated as the cause of academic difficulty, tests are administered by remedial specialists, school psychologists and social workers to determine the presence of specific learning disability (SLD).
Performance and intelligence tests in certain subject areas (reading, spelling, arithmetic, etc.), coupled with observations of classroom behavior and attention lead to the declaration of learning disability.
Such a declaration triggers legal, social, funding and instructional constraints for all concerned. Over the years various strategies such as pull-out, push-in, main streaming and response to intervention (RTI) among many other modifications of curriculum, pedagogy, classroom configurations and student groupings have come and gone with dismal result.
Since the invention of the “diagnosis” of learning disabilities in 1970, the percentage of students receiving “special compensatory” educational services has increased from roughly 2% to 25% of all students. As compensatory education services cost roughly three times that of general education, one can readily understand the graph above.
ICONIX targets underlying visual attention and thinking skills needed to supplant environmental stimuli as the driver of behavior.


The beauty of this approach is visual skills develop naturally when one knows how to ride that train. We identify and eliminate obstacles blocking natural development to visual dominance, fill-in some gaps and encourage natural skill progression by using the greatest instructional method of all-time – Play.
ICONIX is a program and plan designed to assist parents to take direct control of their children’s education. It is a four-suite virtual platform that contains complete diagnostic, proctor, and teacher training and certification, teaching methods, and curricular services coupled with real-time, ongoing online, and onsite support. Each household, classroom, or school is supported by case managers, trainers, and diagnosticians from regional support centers.
Such a declaration triggers legal, social, funding and instructional constraints for all concerned. Over the years various strategies such as pull-out, push-in, main streaming and response to intervention (RTI) among many other modifications of curriculum, pedagogy, classroom configurations, and student groupings have come and gone with dismal result.
Attention deficit hyperactivity disorder is not a disease. Environmental stimuli control attention and behavior of some children more than others. When this tendency is rather arbitrarily deemed excessive, an attention deficit is declared.
A cat chases a laser dot to exhaustion; dot controls cat. He has no internal mechanism to override the controlling influence of the external stimulus. You will not chase dots because you “see” the future and override the external stimulus with your “choice” of behavior.
ADHD is incomplete visual dominance exemplified.
Impulsive verbal and physical behavior is hyper-responsiveness to external stimuli. These behaviors exemplify incomplete emergence of visual dominance. Mind sight overrides external stimuli in a competition for control of behavior.
When vision becomes dominant as it eventually does in all healthy children, they stop “chasing dots”, they start running to where the soccer ball will be instead of where it was; they see the future and choose their behavior - they become more reflective. The problem is how many epigenetic “work arounds” became habituated prior to vision becoming dominant?
Pharmaceutical suppression of awareness of external stimuli may temporarily reduce distraction, but is purely compensatory, metabolically dangerous, and stands in direct opposition to expanded visual development. Fortunately, the “cure” is natural development culminating in visual dominance.
These children do not have a disease, they lack skills - skills that naturally emerge from the very behaviors that lead to the “diagnosis.” Let them play their way out of the behaviors. Change the classrooms, not the kids!

"Fewer drugs, more skills"
...is a better approach.

The reason the “diagnosis” was invented in the first place is that yet-to-be visually dominant children resist classrooms. They just refuse to follow the rules. Turns out they were right all along!
"Fewer rules, more play"
...is a better approach.
Play is the greatest teaching method of all time.

It’s an all too common story...your child starts bright eyed and vibrant. They are full of curiosity and affection. They had just begun to say “Mama.” Suddenly, everything changes. Your baby stops looking at you. Your baby starts doing “odd” things. Your family and friends begin pointing them out. They say, “It’s not normal for a baby not to smile.”; “It’s not normal for a baby to line up their toys like that.”; or, “You should get them checked out.”
After your inner circle points these things out, you finally decide to get some answers. Some tests and a few conversations later...your child has a new diagnosis: Autism. You flash through a new life in your mind—similar to when you imagined your baby in the first place—only this time there is less clarity, less certainty, and less opportunity. Having come to terms with this new idea of how life is going to be, you start to ask all of the questions.

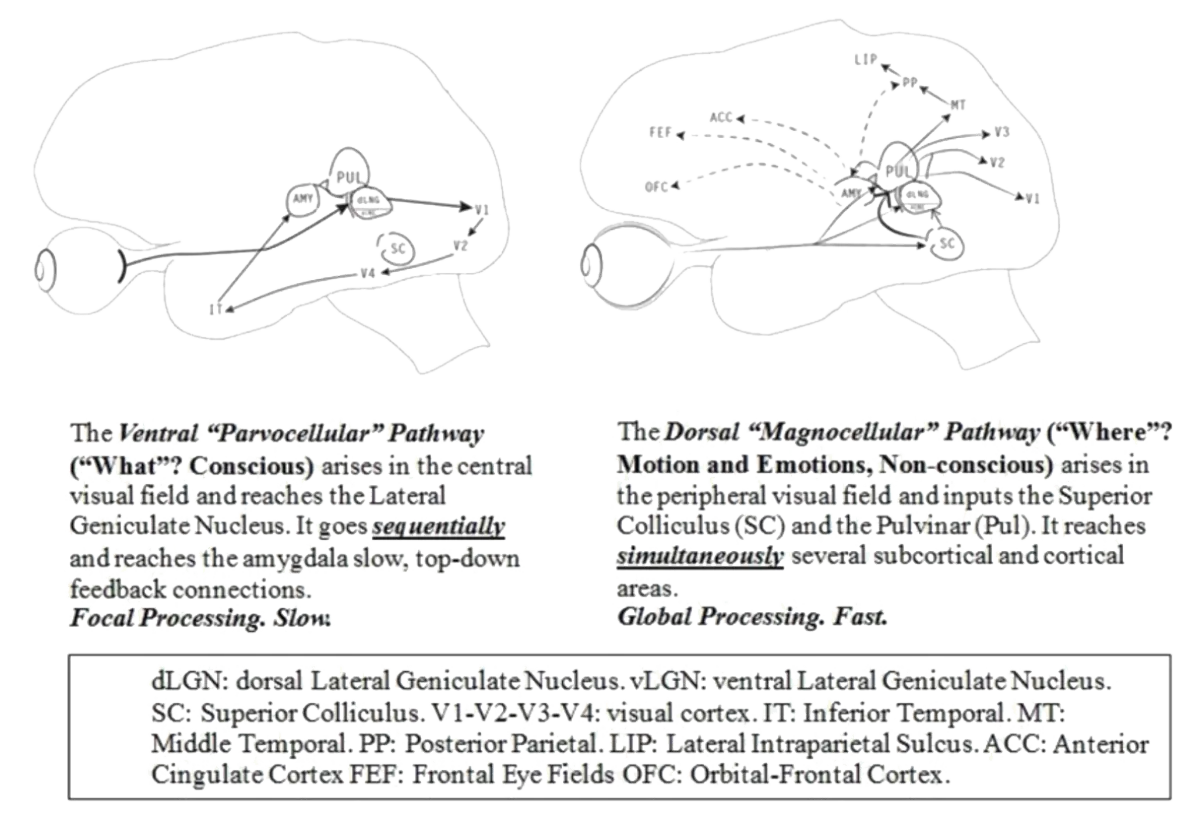
Autism is not a disease, it is a constellation of behaviors associated with atypical visual attention.[citation] Autism is a biphasic epigenetic phenomenon. The first marked by reduced neonatal reflexive magnocellular — mediated eye movements involving the superior colliculus. The second a dramatic regression of parvocellular — striate - ventral stream visual attention that occurs secondary to binocular instability between 15 and 30 months of age.[citation]
Let’s decode that bit of neuro-speak into Lay-speak [lay-speak in green].
Babies come into this world equipped with what are known as infantile movement reflexes sometimes called primitive reflexes. These reflexive movements cause the neonate to move in response to certain environmental stimuli. For example, the asymmetric tonic neck reflex (ATNR) causes a baby to reflexively begin suckling, roll the neck and extend the limbs toward a brush of the cheek. The purpose of the reflex is obvious.
There are several such reflexes that appear and become “integrated’ during early development. Four especially important primitive reflexes involve reflexive eye movements.
These eye movement reflexes cause neonates to follow faces as well as certain motions with their eyes. Children with less robust tracking reflexes are more likely to develop stereotypical autistic behaviors. Babies with “soft” tracking reflexes develop less robust eye teaming coordination.
Their eyes do not “snap” into coordinated alignment as quickly as those with robust tracking reflexes. Tracking reflexes and eye teaming are closely related because they share the same visual pathways.

Binocular stability and reflexive tracking [citation] rely on input from rod photoreceptors in the retinal periphery carried along magnocellular ganglion cells up the superior colliculus integrating visual input with autonomic, endocrine, circadian and emotional functions. Weak eye movement reflexes correlate with delay in executive function (orbito-frontal cortex), binocularity instability (cranial nerves III, IV, VI), visuo-spatial perception (oculo-vestibular-spinal proprioception integration), immunodepression, autonomic imbalance, sleep problems (pineal - circadian rhythms), emotional and endocrine dysregulation (superior colliculus-amygdala-pulvinar complex), pursuit, saccade and anti-saccade eye movements (frontal and supplemental frontal eye fields), and visual-social (mirror cells of the cingulate gyrus) [citation], vocabulary, [citation] language articulation, [citation] hand-eye coordination and qualitative ordering and numerosity (lateral intraparietal sulcus) [citation].
Let’s decode that bit of neuro-speak into Lay-speak
[lay-speak in green].
Weak tracking reflexes lead to less precise eye and hand movements. Unstable eye teaming and abnormal visual attention pervasively impacts sleep, emotional regulation, immune response, respiratory, digestive, cardiac and hormonal fluctuations, organization in time and space, reading of social cues, language, speech articulation and academic performance.
ICONIX diagnosticians are acutely interested in primitive reflexes, especially eye movement reflexes.
Less robust and/or asymmetric optokinetic, end-point nystagmus, oculo-gyral, facial pursuit and vestibular-ocular primitive reflexes are harbingers of depressed magnocellular activation in the ventral layers of the lateral geniculate nucleus, [citation] motion detection in the striate cortex, [citation] and transient system depressions.[citation] Weak eye movement reflexes are positively correlated with severity of stereotypical autistic behaviors.[citation] Resultant spatial perception deficits impede development of stable binocularity; the key etiologic factor underlying the dramatic epigenetic second phase: autistic regression syndrome.

Peri-foveal attention preference to escape diplopia results in relative parvocellular neglect which if habituated results in profound afferent perceptual and efferent functional sequelae. Language, social cues, eye contact and focal attention in general all precipitously diminish as parvocellular neglect habituates. Regressive autism is a parvocellular neglect syndrome paradoxically more common in those with early magnocellular depression. Small angle diplopia and epigenetic compensatory peri-foveal fixation is the pathogenesis of regressive autistic behaviors.
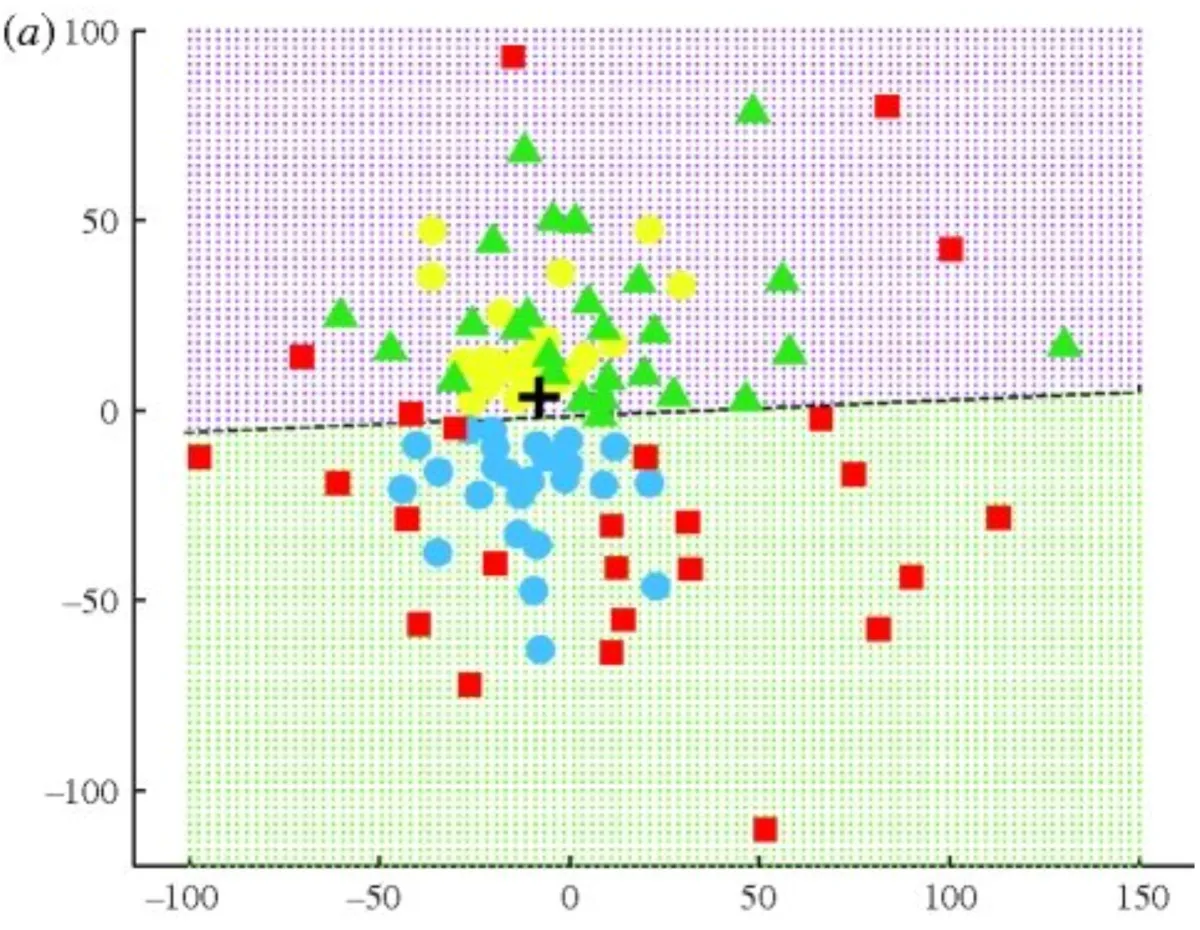
This fixation plot of visual attention in face-to-face social confrontation among neuro-typical (yellow), hearing impaired (blue), attention deficit (green) and autistic individuals (red) maps eye pointing behavior to eyes, mouth, competing environmental stimuli, and peri-foveal alignment, respectively. Eye pointing reveals invaluable diagnostic cues as to the invisible and most defining aspect of all people - their attention and thinking.
Eyes reveal mind.
Stereotypic autistic behaviors such as hand flapping, repetitive light switching, venetian blind flipping, and looking through moving splayed fingers create visual motion which stimulates magnocellular attention to override competing parvocellular input. Children with autistic behaviors attend to space not the items within space.

Autistic children are literally “lost in space” with no attentional anchors. They do not “visually grab” items of interest with their central vision as do neuro-typical children. Binocular stability allows vision to match touch as neuro-typical children “come out of the terrible twos.” Central vision supplants the hand as the primary explorative (grabbing) tool. Autistic children habitually neglect central vision and fail to develop the functions dependent on parvocellular (ventral stream) input, most notably language and social engagement.
All behavior is purposeful. We must understand purpose and from whence it comes as the first step in developing proper instructional strategy.
We now understand the purpose of autistic behaviors - purposeful avoidance of central visual input, parvocellular neglect. Small alignment errors in eye teaming cause double vision in central vision but not in peripheral vision. Stereotypical autistic behaviors include “looking off center, out the corner of their eyes.” This is called peri-foveal fixation. It is a means of avoiding double vision when the eyes are slightly misaligned. Please watch the video below and repeat the experience for yourself to better understand the cause of peri-foveal fixation to eliminate double vision which when habituated results in parvocellular neglect, the main cause of autistic regression.

The first step in naming objects is visually grabbing them with central vision. Once objects are “grabbed” from background, they can be recognized as similar to previously “grabbed” objects. Categorization of objects allows grouping by similar salient features that are then named. Failure to visually grab and separate objects from the background thus stifles language development.
Central and peripheral vision compete for our attention. We cannot “see” both at the same time. We learn to toggle back and forth between these two figure/ground attention systems to make sense of the world. We alternately see both ambient and focal features - forest and trees.
Autism is a near full neglect of focal attention.
ICONIX has designed instructional games, experiences and techniques to excite central visual attention to help children learn to visually grab objects as the vital gateway to language and “reading minds” by looking squarely at faces.
All children who struggle with language, social skills and executive functions need a careful assessment of visual attention because imbalance between central and peripheral vision is a newly understood factor that underpins many learning problems, none more dramatic than autism.
